1. Tested Twice
1. Tested Twice
Vaccines are tested and approved internationally and in South Africa before they are given to people.Oversimplified and misleading. There are two ongoing trials of the Pfizer/BioNTech vaccine, one sponsored by BioNTech in Germany (Phase 1), and another sponsored by BioNTech(Pfizer) in the USA, Argentina, Brazil, Turkey, South Africa and Germany (Phase 1,2,3). Not all phases are completed. None of the trials are independent, and the trial data is not available for public scrutiny. So, we have to rely on the honesty of the manufacturer to provide accurate data. The animal trials failed, so all of these trials are given to the trial participants (people) before they are given to the general public (also people). There were 771 people in phase 1, and 87,495 people in phases 2 and 3. [1]. No "Vaccine safety" information provided.
2. New Technologies
New technologies and information about other Coronaviruses before COVID-19 made production faster.Vague and misleading. Presumably it is referring to the fact that these are mRNA vaccines. The mRNA technology hasn't been successful in any previous attempts at a vaccine. The manufacturers of the vaccine are immune from prosecution for any side effects, manufacturing defects, quality control lapses, or incorrect administration of the doses. For example, in the first 90 days after approval of the vaccine in the USA, 7 people died due to incorrect administration or dosing out of 2792 reported "Medication Error" events. Administration had not even started in South Africa at that point. [2:Page 26]. Again, no "vaccine safety" information, just talk about faster production and new technologies.
3. Over One Million Volunteers
Over one million volunteers were part of the testing process for the vaccine - 2 000 South Africans tested the vaccine.Wrong. NIAID was looking for a million volunteers [3:July 2020] but the Pfizer trial involved 90,000 people at best (see above), and it doesn't say how many South Africans were involved. The Johnson & Johnson trial involved 2,000 participants in South Africa [4], but presumably half of them were in the control group, so they didn't "test" anything. Again, no mention of the safety of the trials.
4. Millions Are Vaccinated
Over 700 million people around the world are already fully vaccinated.Again, misleading. It implies that 700 million people were safely vaccinated, but avoids actually saying that. The real situation is being carefully concealed and manipulated by the drug companies, the "health" authorities, and many doctors (and pharmacists who care). [5] If you are convinced that the vaccine is "safe and effective" then what do you say when a patient dies within 48 hours of taking the vaccine? Who is going to pay for the autopsy? So the doctor says, "it's a coincidence" and doesn't mention the vaccine as cause of death. It happened to a family friend. They are too busy grieving to worry about the doctor's lies. So if you hear that millions are vaccinated but don't hear about the side effects and fatalities, does that mean the vaccine is safe?
5. Side Effects Are Tracked
Vaccines may have some side effects. All vaccine side effects are monitored over time.Once again, this is false and misleading. It implies that "someone" is actively monitoring for vaccine side effects and injuries. Pfizer isn't doing it, and they admit as much. They are passively accepting data sent to them. This data has to be forced out of the FDA by a court order [6] after they sat on the data for months, and claimed it would take years to be released, despite their legal obligation to do so in a timeous fashion.
- Nervous system disorders (25,957)
- Musculoskeletal and connective tissue disorders (17,283)
- Gastrointestinal disorders (14,096)
- Skin and subcutaneous tissue disorders (8,476)
- Respiratory, thoracic and mediastinal disorders (8,848)
- Infections and infestations (4,610)
- Injury, poisoning and procedural complications (5,590)
- Investigations (3,693)
6. Protects Against Serious Illness
You can still get COVID-19 but the vaccine protects from serious illness and death.Where is the data? Most countries with high vaccination rates are still experiencing high death tolls and hospitalization rates. Most media reports try to spin this as "the unvaccinated" are getting sick, but the reality is quite different. One study shows that "Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States" [8]. Public officials are promoting "booster shots" as being necessary because the vaccine's "protection" only seems to last about 6 months. So I guess the death of 1,223 people in 90 days is not a serious death.
7. Check for Side Effects
In the days after your jab, check your body for side effects like tiredness, soreness, headache, fever, dry cough, etc.All of the mentioned side effects are also listed as symptoms of a COVID-19 infection. That's because the vaccine generates the same toxic spike protein found in SARS-Cov-2. But the vaccine generates these toxic proteins in an unregulated way. Notice that none of the serious side effects listed above are included. This is deliberately misleading.
- Relevant event seriousness: Serious (2341), Non-Serious (617);
- Gender: Females (876), Males (106), Unknown (20);
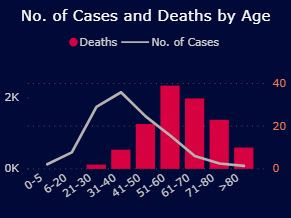
- Age (n=961) ranged from 16 to 98 years (mean = 54.8 years, median = 42.5 years);
- Relevant event outcomes: fatal (9), resolved/resolving (1922), not resolved (229), resolved with sequelae [complications] (48), unknown (754).
8. Works in Two Weeks
The vaccine will take two weeks before it gives protection against COVID-19.Again, what is NOT said is more important than what is said. During those two weeks your immune system is temporarily compromised as it deals with the unregulated production of the toxic spike protein. So any conditions that you may have had in the past that were being suppressed by your immune system can flare up again. Also, you could get flu, COVID-19 or any other contagious disease if exposed to it during that period, and your body will probably battle to deal with both at the same time. But in many regions you aren't classified as "vaccinated" until after the two week window, so any problems that occur during that time may well be recorded as occurring in "unvaccinated" patients. That's how the data is skewed. Here is the CDC definition: "For the purposes of this guidance, people are considered fully vaccinated for COVID-19 ≥2 weeks after they have received the second dose in a 2-dose series (Pfizer-BioNTech or Moderna), or ≥2 weeks after they have received a single-dose vaccine (Johnson and Johnson) ... Unvaccinated people refers to individuals of all ages, including children, that have not completed a vaccination series or received a single-dose vaccine." [9]. Again, no safety data, just a bland statement that the vaccine works (assuming you survive the two weeks).
9. Stay Safe
You can spread COVID-19 to people not vaccinated. Wear your mask. Sanitize. Social Distance.What? Let's unpack this a bit more: since you are presumably vaccinated, you got COVID-19, which means you can catch it from people who are vaccinated, and likewise spread it to people who are vaccinated. So why only mention people who are not vaccinated? This is blatantly dishonest from the "pharmacists who care".
10. Tell Your Family and Friends
Tell your friends and family about your experience and encourage them to get vaccinated.Yes, I got suckered by this one. I told my community that I didn't experience any bad side effects, just tiredness and a sore arm. I learnt back from my community that one person had a stroke, and another suffered pericarditis. My brother told me about a friend who had a bad reaction within 24 hours, went to hospital, and died within 48 hours. Of course, it had ABSOLUTELY NOTHING to do with the vaccine. Because the doctor said it was so. People just drop dead all the time for no reason. My niece's husband who isn't even 30 has been having heart palpitations. It was unusual in his age group until the pandemic came along.
So what should we make of the lies and disinformation in a single poster? It seems to me that the "Vaccine uber alles" brigade will go to any lengths to "nudge" people to get a vaccine that is ineffective at best (the pandemic isn't over in countries with high vaccination rates) and dangerous at worst. The mRNA vaccine manufactures toxic spike proteins in the body in an unregulated manner, so they can spread around the body and cause havoc with just about every part of the human body. What could possibly go wrong?
Update 17 December: Unvaccinated employees must get vaccinated or be subjected to weekly tests, at their own expense. And they must wear expensive N95 masks. Dr Verwoerd would have been so proud of this version of #VaccineApartheid.

Update 18 December: I found some expensive "Civilian KN95" masks at one of their stores (but not online).



I could only find one mask that doesn't use the ear loops (R70), but instead has ties that you can use to tie behind your head, like the ones that surgeons use. Pathetic.
Update 14 January 2022: DisChem has managed to get itself on the red list and face a consumer boycott. And then there's this:

Update November 2022: Last year they lied about the vaccine. This year their board turned racist and announced they would no longer be hiring any new "whites" to meet their racist "diversity targets". The most glaringly non-diverse part of their organisation is the senior management, whose 5 male "executive directors" seem to be exclusively "white", and their 5 "non-executive directors" aren't. I wonder whether these "non-executive" directors really have any say in the running of the company, or whether they just feel they are token appointments, based soleley on the colour of their skin. So now their new motto should be: "Dis-Chem: pharmacists who care; management that doesn't."